

So we're going to do a series that goes over prehospital blood products, primarily for use in trauma. We'll be breaking down what's inside blood, what the different components are, how it's stored, how it's administered, and some of the advantages and disadvantages of each.
Whole Blood Vs. Components
Blood and blood products can either be given as whole, so whole blood, or it can be given as components. Again, those primary components are red blood cells, platelets, and plasma. There are advantages and disadvantages to each, but in general, what we're trying to do is match the capabilities of whole blood when we give it prehospital or even in the hospital for resuscitation.
Years ago, blood bankers and physicians discovered that you can break up whole blood into different components. That created somewhat of an advantage as far as supply chain goes and differences within storage. It was also thought that you could customize your treatment of the patient. So if they needed platelets, you could give more platelets. If they needed red blood cells because anemia was the main problem, then you could just give red blood cells and make that bag of whole blood or that unit of whole blood last even longer.
Red Blood Cells
So let's talk about what some of those components are. Red blood cells, or RBCs, are one of the primary components in blood. What they do is deliver oxygen from the lungs to the tissues. The red blood cells pick up oxygen at the lungs, and then they transport it to the tissues, your organs, where that oxygen is dropped off at the organ, and then that organ now has oxygen. It also takes CO2 from those tissues and transports back to the lungs so you can off-gas or exhale that CO2.
This maintains a balance of oxygenation. It also helps with pH balance from CO2. Red blood cells are primarily stored within a plastic bag with a preservative in them. For the most part, red blood cells last 42 days and need to be kept refrigerated.
Freezing Red Blood Cells
There are also ways that you can freeze red blood cells for long-term use. The military does this, and they store massive amounts of them, and they can store for 10-plus years. The issue with that is that it takes a long time to not only thaw them, but you have to wash the glycerol off of the red blood cells, which is a very technical process and takes some time. So it's really not practical for prehospital use, but it's great for contingency planning, where you may need large amounts of red blood cells.
The Fresher, The Better
As you store red blood cells, the fresher they are, the better they're going to work. So, as red blood cells age, they decrease in quality and effectiveness over time. So a day one red blood cell is going to be a lot better than a day 42 red blood cell. Why is that? Well, that's because as red blood cells age, they get what's called storage lesions.
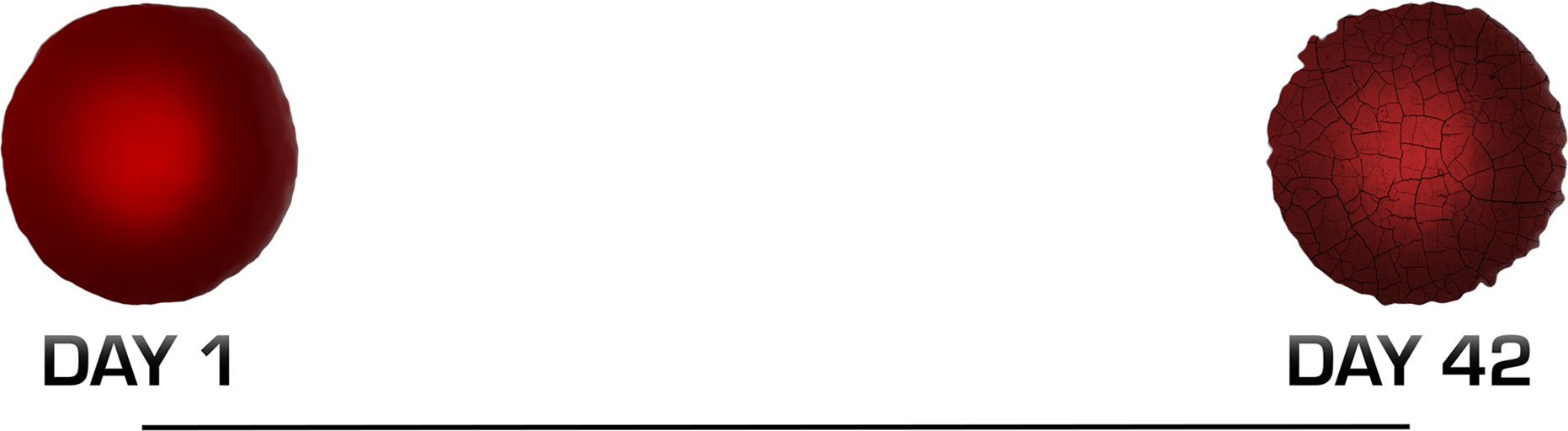
This affects the structure and the function of that red blood cell, so it's not going to carry oxygen as well, it's not going to last in the circulatory system as long, and it's going to break down quite a bit easier and quicker. It's not going to be as functional as a newer blood cell. So what you're going to see with blood products in general, the newer they are, the better they're going to function, and then they lose function over time to a certain point where we say, "You know what? That's no good. Enough of those red blood cells have broken down, and we're not going to use them anymore."
Blood Typing
One of the other issues with red blood cells in the prehospital environment is that you need to pick out the donor to match the recipient. In general, rather than trying to type your patient at the scene, what we do is a universal blood cell, which is a type O blood cell.
Ideally, it's going to be an O negative, which means it's Rh negative for females of childbearing potential, and that's just to prevent complications in the future from pregnancy.

Transfusing Red Blood Cells
Finally, red blood cells can either be transfused by themselves, which the downside is they lack the platelets, they lack the proteins, and the clotting factors in plasma, and you're not going to get that volume. So you're going to get blood delivery, but it's not necessarily going to help with clotting, maintaining clots or even increasing blood pressure that much if that's really what your goal is.
